MRCS Knowledge: Large Bowel Obstruction
23/10/14 20:39 Filed in: MRCS Knowledge
MRCS Part B Knowledge: Large Bowel Obstruction

Today’s MRCS Knowledge short notes are on Large Bowel Obstruction.
Background
Mechanical or functional obstruction of the large bowel, preventing the normal transit of the products of digestion
Aetiology
Causes of Large Bowel Obstruction:
Intraluminal
Gallstone ileus
Food/Faeces
Intussusception
Bowel Wall
Strictures
Tumours
Diverticulitis
Extraluminal
Sigmoid/caecal volvulus
External Compression
Signs and Symptoms
- Abdominal distension
- Generalised abdominal tenderness
- Tinkling bowel sounds
- Palpable mass
- Empty rectum on PR
- Constipation
- No flatus in complete obstruction (flatus in partial obstruction)
- Generalised abdominal pain
- Late onset vomiting
- Dehydration
Investigations
- Bloods: FBC, U&Es
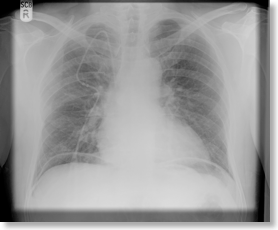
- Erect CXR: looking for air under diaphragm indicating perforation (see below)
- AXR: central, dilated loops of large bowel, >5cm (distinguished by haustral folds which partially cross bowel diameter)
- CT Abdo: identify level and cause of obstruction
- Gastrograffin follow-through: identify level and cause of obstruction
Management
Immediate: NBM, nasogastric tube and IV fluids ‘drip and suck’, urinary catheter to monitor fluid balance. May not be adequate as the large bowel produces around 9L of fluid per day
Treat underlying cause e.g flatus tube for volvulus
If no improvement may require surgical resection +/- resection with temporary colostomy
Prognosis
Complications: Perforation (in 20% patients ileocaecal valve remains closed increasing pressure on thin-walled caecum leading to perforation), peritonitis, severe dehydration, death
Further Info:
For further info and commonly asked questions on large bowel obstruction be sure to sign up to the Question Bank.
blog comments powered by Disqus